BENIGN BREAST CONDITIONS & BREAST PAIN


Breast pain
Breast pain is very common in women in reproductive age group, and on its own is never a sign of cancer! In other words, if breast cancer is a cause of breast pain it is invariably associated with other more obvious signs and symptoms such as ulcerating lumps, redness, peau d’orange, …
Many women present with breast pain and often all they require is reassurance and intermittent Panadol or anti-inflammatories as needed. In those with ongoing daily pain we recommend reduce caffein and tea intake, well fitted bras, and daily evening primrose oil tablets (up to 3 a day) ± vitamin B6.
Breast Infection/Mastitis
Mastitis refers to breast inflammation. It is most commonly due to breast infection however it could also be due to non-infective causes. The local symptoms include breast lump, redness, pain and tenderness. It may also be associated with systemic symptoms such as fever, chills and body aches and pains.
Lactational mastitis
This is the most common type of mastitis which is seen in breastfeeding women. The cause is blocked mild duct which is often due to inspissated milk caused by infrequent feeding. The blocked mild duct then becomes a perfect culture medium for secondary bacterial infection.
Periductal mastitis
This is the second most common cause of mastitis seen almost exclusively in smokers. It is postulated that smoking damages the subareolar ducts leading to blockage and subsequent infection.
Granulomatous mastitis
This is an idiopathic (unknown cause) recurrent mastitis often seen in parous young woman often form the Indian subcontinent or middle east or Hispanic descent. The inflammation is associated with multiple masses, skin erythema/ulceration. As radiological findings can mimic cancer, core needle biopsy is often required to confirm the diagnosis.
Benign Breast Lesions
Breast Cysts and Fibrocystic Changes
Cysts are commonly found on breast ultrasound. Simple and complicated cysts have no risk of malignancy and unless large and symptomatic do not need treatment or follow up. Large palpable cysts can be aspirated to relieve symptoms and facilitate future self-exam.
Most so-called complex cysts are indeed simple or complicated cysts with no malignant potential. True complex cysts often need biopsy or follow up depending on the ultrasound features. Remember ultrasound is very operator dependant. Seeing an experienced breast surgeon with ability to perform bedside ultrasound is the best next step to provide second opinion on the reported ultrasound and advise the next step.
Fibroadenoma
These are the most common benign breast lesions often seen in young women between 15 and 35 years of age. A hormonal aetiology is possible as they often grow during pregnancy and regress with menopause. There is no increased risk of breast cancer with these lesions and treatment is guided by symptoms and size.
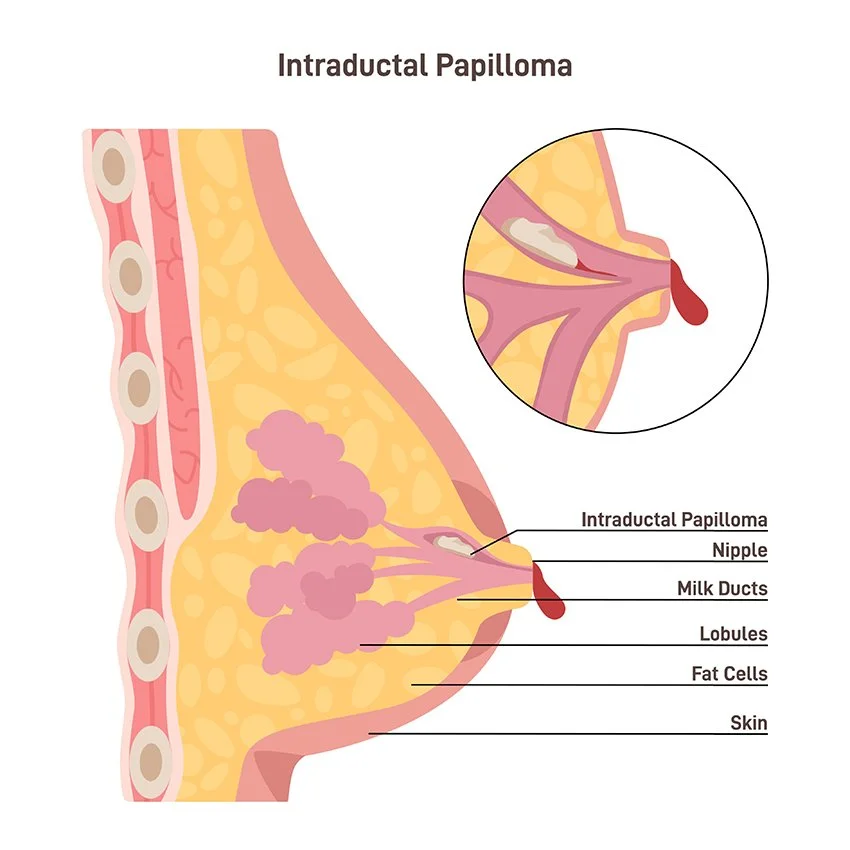
Intraductal papilloma
Think of these lesions as little polyps arising from the milk ducts lining. Although benign, excision is recommended as they can harbour cancer cells within them or develop into breast cancer in the long run.
B3 Lesions
These lesions are incidentally discovered on core needle biopsy specimens, and although not malignant (cancerous) per se, they have uncertain malignant potential and therefore excision is recommended. Some of the more commonly seen B3 lesions include atypical ductal hyperplasia (ADH), atypical lobular hyperplasia (ALH), lobular carcinoma in situ (LCIS), radial scar, complex sclerosing lesion, and papillary lesions.
Nipple Discharge

Nipple discharge is a very common breast symptom, mostly physiological, occasionally pathological, and only rarely associated with underlying cancer specially in women < 40 years of age.
Physiological nipple discharge or galactorrhea could be unilateral or bilateral (both breasts) and most-commonly caused by nipple stimulation or medications (antipsychotics and antidepressants). Occasionally it may be caused by a benign pituitary tumour producing prolactin hormone (the milk hormone normally secreted during breastfeeding).
The two most common causes of pathological nipple discharge are intraductal papilloma and duct ectasia. The former is a benign growth within a milk duct associated with unilateral clear or bloody nipple discharge, while the latter is referred to dilated subareolar milk ducts associated with often bilateral greenish or cheesy discharge.